

Originally published in Volume 42 Issue 5 of Artificial Organs, 16 May 2018
Could a mechanical heart be built? One that would be good enough to use clinically? How fanciful was this idea, and, if taken on, how best to go about it?
In the late 1950s and 1960s, three different devices demonstrated the feasibility of mechanical hearts and validated a multiple approach strategy to the development of this technology. Dutch-American physician-researcher Willem Kolff and Japanese medical researcher Tetsuzo Akutsu built a total artificial heart (TAH), Texas surgical titan Michael DeBakey developed an external bypass-type ventricular assist device (VAD), and cardiothoracic surgeon-investigator Adrian Kantrowitz experimented with an implantable “booster heart” or serial-type VAD. Was one approach better than another? Who would be first in delivering a workable device, and would firstness ultimately decide the better research direction to pursue?
In Cleveland, Ohio, Kolff and Akutsu pursued the development of a total artificial heart as a permanent mechanical replacement for a removed, failing human heart. Before coming to the United States, Kolff had built a workable artificial kidney machine, and he transferred that knowledge of and experience with blood flow to his mechanical heart research. Still, building a total artificial heart was an ambitious tactic. Kolff and Akutsu completed 27 experiments of implanting plastic valves in the hearts of dogs before they boldly jumped ahead to build an entire plastic heart, composed of two polyvinyl chloride pumps (Fig. 1). It was a pneumatically driven device, built from a plastic cast impression of the heart of a 60-pound dog. The heart was connected to an air compressor by plastic tubes. This air-driven heart was tested first in mock circulation on the bench (to ensure mechanical function), then implanted into a dead dog (to study surgical procedure and fit), and finally placed into a living dog in December 1957. The dog lived for 90 min with the implanted heart before device complications terminated the experiment 1.
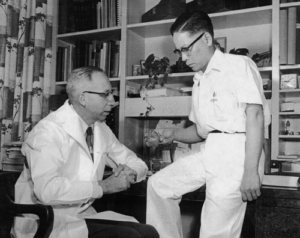
Figure 1
Kolff and Akutsu promptly reported their experimental animal case to the professional community, eager to claim it as the first successful TAH implant in an animal in the Western world. (Years later, Kolff and Akutsu learned that a Soviet scientist, Vladimir Demikhov, had performed a similar experiment in 1937.) In their opinion, the experiment was a success because their device had functioned in vivo (in animals), keeping the dog alive for 90 min, and it was cited as such in medical textbooks thereafter. For Kolff and Akutsu, it was proof of concept. While it might have demonstrated the feasibility of mechanically maintaining circulation for a limited time, the device was certainly not successful enough to be implanted in humans. The efficacy of the device was questionable, given that the dog had hardly moved from the operating table.
In Houston, Texas, DeBakey also came to the endeavor with experience building mechanical devices that interacted with the blood; he had invented the roller pump used in John Gibbon’s heart-lung machine and was investigating the viability of artificial arteries for vascular bypass procedures. His initial approach to a feasible artificial heart focused on developing ventricular assist pumps for temporary assistance as a bridge to surgical recovery. This was a more realistic aim, driven from the operating room and aimed at clinical utility for extended mechanical support beyond the heart-lung machine. DeBakey’s research team, which included cardiac surgeons C. William Hall and Domingo Liotta among others, developed a variety of mechanical pumps including an external bypass-type ventricular assist device 2.
This external bypass-type device was most likely the sixth DeBakey model. Unlike the other pumps, this device rested outside the body (paracorporeal), with two connecting tubes (for blood flow) penetrating the patient’s chest to attach to the left atrium and a systemic artery. The hemispherical, pneumatically driven pump was made of Dacron-reinforced Silastic with a molded diaphragm separating the gas chamber from the blood chamber. Pressurized air pulsed into the gas chamber, which collapsed the blood chamber and pumped the blood into the systemic artery for circulation into the body. DeBakey viewed this device as temporary, to be used for only a matter of days or weeks, so placing the pump outside the body permitted easier surgical implantation and removal. In August 1966, he implanted the pump in 37-year-old Esperanza Del Valle Vasquez, whose weakened heart had failed to resume function after aortic and mitral valve replacement surgery. After 10 days, DeBakey assessed the patient’s heart to be strong enough to pump on its own, and he removed the device. The patient made a full recovery and was discharged from the hospital one month after her valve surgery 3. Thereafter DeBakey reported more clinical cases, in which other patients also benefited from short-term pump assistance after heart surgery.
In Brooklyn, New York, Kantrowitz applied his theory of diastolic augmentation (or synchronized arterial counterpulsation) in the development of several cardiac assist devices or “booster hearts.” In contrast to DeBakey’s bypass-type pumps, which pumped independently of the heart and reduced blood flow by the natural heart, Kantrowitz’s serial-type devices worked in tandem with the heart and augmented the natural heart’s blood flow. Kantrowitz’s device was smaller than DeBakey’s pump and had no valves; it was intended for permanent use, operated continuously or intermittently, and was placed inside rather than outside the body. Kantrowitz’s device was a sausage-shaped double tube—a flexible silicone-rubber inner chamber encased in rigid fiberglass housing—with woven Dacron cuffs that connected surgically to the ascending and descending aorta. Its surgical position along the aortic arch formed the device into a U shape. The inner tube filled with blood during the systole phase of the natural heart. Compressed air then entered between the tubes, expelling blood from the inner tube into the circulatory system during the diastole phase of the natural heart. Kantrowitz tested his assist device on 74 dogs over a period of several years to perfect the device, in the process attracting numerous researchers, including Japanese surgeon Yukihiko Nosé, to join his team 4.
In February and May 1966, Kantrowitz implanted his “booster heart” in two patients at Maimonides Hospital in New York. The first patient was a 33-year-old man with chronic left ventricular failure caused by cardiomyopathy, who died less than 24 h after implantation of the device. Two months later, Kantrowitz implanted the device into Louise Ceraso, a 63-year-old woman in congestive heart failure who survived 12 days. The assist device operated intermittently—on for 2 h, off for 1 h. Yet the patient died, from a cerebral vascular event that on postmortem examination proved to be the result of a thrombus originating at the site where the device connected to the aorta 5, 6. Kantrowitz encouraged the use of mechanical pumps in more clinical cases, returning to the laboratory to improve his device before he proceeded.
These three devices–Kolff and Akutsu’s total artificial heart, DeBakey’s external bypass-type VAD, and Kantrowitz’s “booster heart”–differed in size, shape, how they worked, and intended clinical use. Collectively, these multiple approaches helped to sort out best biomaterials, device mechanics, implant tolerance in the body, and other issues. Their work provided greater clarity surrounding the requirements and needs for building artificial hearts. The three research teams were united in their commitment to the feasibility and desirability of artificial hearts, but none of these devices were ready for widespread clinical use.
* This piece is adapted from Shelley McKellar’s recently released book, Artificial Hearts, published by Johns Hopkins University Press in 2018.
* Many of the devices developed in the research programs of Willem Kolff, Michael DeBakey, Adrian Kantrowitz, and others reside in the medical sciences collection at the Smithsonian Institution’s National Museum of American History in Washington, DC.
Biography

Professor Shelley McKellar is the Hannah Chair in the History of Medicine at the Schulich School of Medicine and Dentistry at Western University. She is also an Associate Professor in the Department of History. Her research focuses on the history of surgery, medical technology and the material culture of medicine. She is the author of several books and articles, including the newly-released book Artificial Hearts: The Allure and Ambivalence of a Controversial Medical Technology by Johns Hopkins University Press in 2018.