Originally published in Volume 42 Issue 2 of Artificial Organs, 13 February 2018
It was July 1956 and I was ready to start a research fellowship at Cleveland Clinic Foundation (CCF) in Cleveland, OH under Dr. Willem Kolff (Fig. 1). As a Japanese exchange fellow, I was excited but scared to be working with such a prominent researcher. In 1944, he had invented the first clinically successful rotating drum artificial kidney (RDK) 1 (Fig. 2).

Figure 1
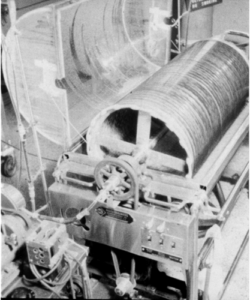
Figure 2
Dr. Kolff was born on February 14, 1911 in Holland. He graduated from the University of Leiden Medical School in 1937 and received his PhD from the University of Groningen in 1946. He married Janke Huidekoper in 1937 and they had five children.
In 1941, Dr. Kolff worked at an 80-bed city hospital as a junior physician in Kampen, Holland and was assigned to four beds on the medical floor. One of the patients was a young man dying of end stage renal disease (ESRD). The patient was an only child and his father had died years earlier. His aged mother visited him every evening after working at the farm. Dr. Kolff had to tell her that he could no longer help her son and he would die soon. He felt he was worthless. It was then he realized he needed to find a solution to prolong the lives of patients with ESRD.
Dr. Kolff thought if he could remove uremic toxins and body fluids that were accumulating in such patients with an apparatus, then the patient would be able to live longer. He paid a visit to biochemistry professor Richard Brinkman at University of Groningen, who was studying osmosis using cellophane membranes. He suggested to use it for dialysis. Dr. Kolff conducted an experiment using 250 mL of blood containing 200 mg/dL of urea in a piece of cellophane casing 5 cm in diameter attached to a wood board. He then submerged the casing in a rectangular container filled with normal saline and shook it up and down by hand. To his surprise, within 5 min almost all the urea was removed. He then calculated that he would need a 20-m cellophane tube to make an effective artificial kidney (AK).
With that data, he asked for technical help from an engineer H.Th.J. Berk who was the director of an enamel company. They had constructed a few AKs without success and then invented the RDK in 1944. They wrapped 20 m of cellophane sausage casing on the drum which operated at 28 rotations/min. It was partially submerged in a receptacle containing 100 L of normal saline. The cellophane tube filled with the patient’s blood would come in contact with the saline solution. To prevent twisting of the cellophane tube at the connecting joints to the drum, he adapted an old Ford car water pump. One drawback was that fluid could not be removed by hydrostatic pressure because the cellophane tube was not protected to tolerate pressure. The fluid was removed by osmosis adding a large amount of glucose in dialysate. Consequently, many patients developed hyperglycemia and needed insulin therapy.
Between March 1944 and July 1945, Dr. Kolff conducted experimental dialysis with the RDK on 15 ESRD patients in Holland and none of them survived. The first survivor was a 67-year-old women who was treated with dialysis on September 11, 1945. He saved her because of his firm conviction regarding equality of the human race.
Close to the end of World War II, he had constructed 4 RDK which were stored in Kampen. After the war, he donated one each to British Post Graduate School in London, Mount Sinai Hospital in New York City (NYC), and the Royal Victoria Hospital in Montreal, Canada. A fourth one disappeared into Poland.
In 1947, Dr. Kolff was invited by Dr. Isidore Snapper to give a talk at the Mount Sinai Hospital in NYC. He received a $300 honorarium. Dr. Snapper introduced him to the Brigham and Women’s Hospital in Boston. Dr. George Thorn, Chief of Medicine at Brigham and Women’s Hospital recommended him to the Arts and Science Society and at Dr. Thorn’s request Dr. Kolff was made an Honorary Member. That membership carried a reward of $3600. He and his wife decided to travel around the United States for 3 months. Upon their return to Holland, Dr. Kolff decided to immigrate to the United States so he and his children would have greater opportunities for success. In 1949, he again visited the United States and met Dr. Irvine Page at the newly expanded Hypertension Research Institute at the CCF. He saw this as the opportunity he had dreamed about and applied for a position. He was hired.
In 1950, Dr. Kolff started to work at CCF. From January 1950 to May 1956 all dialysis sessions were performed with the RDK at his laboratory. However, there was a logistical problem transporting the patients to and from the laboratory. There were three steps and a 90° angle between the sixth floor of hospital and the sixth floor of the research buildings. It was impossible to carry the patient on a stretcher. Thus, two fellows carried the patient in their arms to get there and back.
In early 1950s, no nurse or technician was available for dialysis and the fellows did everything for the dialysis procedure. This included checking the patient’s vital signs, weighing each chemical in a paper bag, and making the dialysate. After dialysis, the fellow cleaned the dialysis tank and the room. The routine dialysis was 6 h and dialysate was exchanged every 2 h. The standard dialysate contained sodium 138, chloride 103, bicarbonate 35, calcium 5, and magnesium 1.5 mEq/L. Only the potassium concentration varied from 5, 3.7, 2.5, and zero mEq/L depending on the patient’s potassium level. To avoid mistakes making the dialysate three steps were taken. The first one was an iron rule. Only one fellow made the dialysate and collected each empty paper bag at the end of dialysis. The second was that several drops of the patient’s blood was mixed with dialysate in a small test tube which was centrifuged; no hemolysis meant the right concentration. The third was a fellow who tasted the dialysate for salt. No osmometer was available then.
In 1953, Dr. Kolff got an idea of performing an arrested open-heart surgery by injecting a high concentration of potassium chloride (KCl) into the base of the aorta after clamping it 2. Dr. Donald Effler, then Chief of Thoracic Surgery, did this experiment on dogs and it succeeded. Then, he applied it to a patient. After connecting a patient to a heart-lung oxygenator and clamping the base of aorta where he injected the KCl solution, the heart stopped and the open heart surgery was performed on an arrested heart. As soon as the clamp was released, the heart promptly restarted its normal regular beats. This revolutionized open-heart surgery around the world.
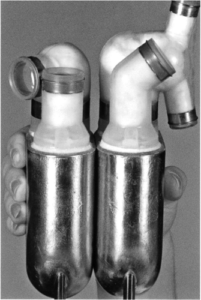
While the dialysis records from 1950 are missing, a total of 62 dialysis sessions were done with the RDK from January 27, 1951 to May 23, 1955 at Dr. Kolff’s laboratory. It was very cumbersome and time consuming to assemble the RDK, so it was rarely used at other hospitals in the nation. He recognized the need for a disposable, ready-made AK. He got the idea of making a disposable twin coil kidney (TCK) (Fig. 3) from the “Pressure Cooker Kidney” made in 1953 by Drs. W. Inouye and J. Engelberg 3. In 1953, he invented the TCK with help from fellow Dr. Bruno Watchinger from Vienna, Austria and Dr. Victor Vertes from Mt. Sinai Hospital in Cleveland 4. He bought a sewing machine for $100 from the Bobbie Brook’s garment manufacture in Cleveland and an engineer adapted it to sew two layers of plastic window screens with two 10 m lengths of cellophane tubing in between. The mesh was then coiled around an empty 10 cm diameter juice can. The initial TCK was made by a technician at his laboratory (Fig. 4). The TCK was sterilized with ethylene oxide gas and aerated for several hours. A Sigma motor was used to pump the blood inside the cellophane compartment and another circulating pump below the dialysate tank would pump the dialysate through the plastic mesh. Because of the tight compartment created by sewing the plastic mesh, it was possible to use a pump to circulate the blood and, therefore, remove fluid by hydrostatic pressure.

Figure 3

Figure 4
On May 27, 1955 the first dialysis was done with the TCK and thereafter all dialyses were done with it. From May 27, 1955 to the end of 1957 a total of 255 dialyses were done. As the number of dialysis sessions and patients increased rapidly, in the middle of 1956 a room in the hospital was assigned to dialysis and two dialysis technicians were hired. The obvious next step was to patent the TCK. Dr. Kolff requested permission from the CCF administration to do it but it was denied. He then contacted the Baxter Company in Chicago, a reputable commercial medical device company, to mass produce the TCK. In the agreement, Baxter would not pay cash but give him one free TCK per every two purchased. The first commercially available disposable AK became available in 1956. Baxter packaged the product so that a 100 L stainless tank and the Sigma blood pump were included with the first purchase. The price of a TCK was $60. This prompted worldwide use of the TCK; however, the interest dwindled due to lack of knowledge in working with it. With Dr. Kolff’s help, Baxter started a training program to help physicians around the world to be able to treat their patients safely.
In the decade of 1950–1960, it was estimated that 50 000–90 000 patients died of ESRD yearly in the United States. Only one dialysis machine was available in all dialysis centers in the nation including CCF. The TCK had two separate and distinct blood channels, so a fellow, Dr. Haakon Ragde, got the idea of using each individual compartment to dialyze two patients at the same time 5. However, this maneuver reduced the efficiency of the TCK in half. From this, I got the idea of dialyzing two patients simultaneously in 1962 by using two separate TCK holders connected to the original dialysate circulating pump. Thus, two patients were dialyzed at the same time provided the dialysate was refreshed every hour. As cellophane’s pores will not permit bacteria or virus to cross, there was no fear to transmit a disease from one patient to another.
In the decade of 1960–1970, there was a preoccupation with the increasing number of the patients who developed ESRD. In 1960, Dr. Belding Scriber in Seattle recognized that permanent access to the blood circulation would be necessary if we were going to attempt to treat those patients. To solve that problem he, with the help from engineer Wayne Quinton 6, created a plastic arteriovenous (A-V) shunt (Fig. 5) to be placed in both the radial artery and cephalic vein of the forearm above the wrist that would provide chronic access. It worked in spite of the opinion of the skeptics. This device made possible the start of chronic dialysis and later kidney transplantation was possible. Dr. Scribner was a longtime friend of Dr. Kolff. When I was sent to Seattle for 1 week to learn the technique, Dr. Scribner kindly invited me to stay at his home.
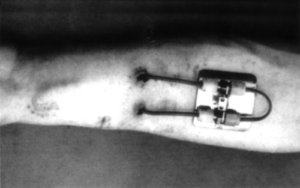
Figure 5
In 1960, Dr. Scribner started repeated dialysis using the Skeggs-Leonard flat kidney 7. He attended the first International Nephrology meeting in Prague, Czech Republic. On the way home, he visited Dr. Kiil in Sweden who invented a flat AK in the late 1950s 8. As the Kiil kidney had a low blood flow resistance, it could be operated without a blood pump. Dr. Scribner thought it was an ideal AK for repeated dialysis. He bought it but it was too expensive to send it by air cargo. He exchanged his airline ticket for a boat ticket. Upon arriving in NYC, he called and told Dr. Kolff that he bought an ideal chronic dialysis kidney from Dr. Kiil.
In 1960s, it was estimated that 90 000 patients died of ESRD every year in the United States. It was technically and financially prohibitive to dialyze that many patients at the dialysis centers. A home dialysis program was started to keep more patients alive. It started in Seattle in 1961 and in Boston in 1964 9. In January 1975, the National Dialysis Registry reported that 12 977 patients were on chronic dialysis. Of those, 3712 patients were on home dialysis. At CCF, the first patient started home dialysis in June 1966 and three other patients started in the same year. From January 1967 to December 1973, a total of 125 patients were trained and started on home dialysis at CCF 10. Dr. Kolff started morning conferences promptly at 8:30 am and ended at 9:00 am. All fellows, technicians, a secretary, a test tube washer, and even visitor(s) had to attend on time. The fellow who did emergency dialysis during the night was excused. For the first 5 min, each fellow took a turn and presented interesting subjects not necessary related to medicine. On my turn in 1964, I spoke about the newly constructed Japanese bullet train. Then, the fellow on call reported his activities during the night. The rest of the time was used by Dr. Kolff to discuss that day’s research activities and he assigned each fellow his duties. One morning, a very distinguished visitor showed up at 8:35 am. Dr. Kolff made him aware that he was late and he apologized. He was an eminent professor of medicine at a famous medical school in NYC. Dr. Kolff established the Department of Artificial Organs in 1958 which was divided into three sections: The first was the clinical section which took care of patients including dialysis. In 1950s, the fellows were Shigeto Aoyama, Maurice Black, Masaktu Shibagaki, Visth Sitpriza, and Satoru Nakamoto; the second was a total artificial heart project with Drs. Ed Miller and Ted Akutsu as surgeons; and the third the heart and lung oxygenator project for open-heart surgery operated by two technicians. Dr. Kolff hired Dr. William Kelemen in 1957 as a clinical associate. Since then Dr. Kolff made ward rounds every Monday and Thursday morning. His main interest was the construction of a total artificial heart (Fig. 6). He employed an engineer, Steven Topaz, to assist with the Artificial Heart project. After moving to Utah in June 1967, he continued the Artificial Heart project in collaboration with Dr. Robert Jarvik where the first artificial heart was implanted in a human. Figure 6 Dr. Kolff emphasized the futility of basic experimentation unless it led to an advancement in the treatment of humans. This was the kind of pragmatism that guided my teacher. However, he would not discourage ideas of young investigators. That is why in 1961 a fellow, Dr. Jerry Rosenbaum, and I told him about the idea of adsorbing urea using a sephedex gel and he allowed us to do the experiment which failed. He told us that a similar experiment earlier had failed and he wanted us to do it. Jerry went back to his home town in Philadelphia in 1962 and succeeded in making an absorption device 11. It became commercially available and was useful especially for patients who had taken an overdose of sedatives or tranquilizers, which were bound to serum protein and cannot be removed efficiently by dialysis. Dialysis grew exponentially in the world. At CCF in 1956, a total of 110 dialysis sessions were performed. In order to keep each patient’s dialysis record in order, Dr. Kolff invented a manual Dialysis Report Card in 1956 (Fig. 7) containing 174 data points for each dialysis on each patient. By punching holes for each data point in each patient, one could easily pull all the cards of patients to whom the data point was relevant. We used an ice pick to pull the relevant cards. These cards made it easy to collect data to evaluate the common problems and also to publish scientific papers. I called it a poor man’s computer. Figure 7 Several other interesting activities occurred under my mentor and I would like to bring some of them up in this report: Dr. Kolff was an innovative and pragmatic man. When I attended the meeting of the American Society for Artificial Internal Organs in Atlantic City in April 1961, I found out that Dr. John Merrill and his group at the Brigham and Women’s Hospital had done successful kidney transplants starting in 1956 with identical twins, later from related living and cadaver donors 13. Though chronic dialysis kept the ESRD patients alive, they had many clinical problems including retention of water and potassium which often required an emergency dialysis. In the middle of 1962 after seeing their problems on ward rounds, I went to Dr. Kolff and suggested that we should start a kidney transplant program. I thought being the inventor of RDK, he would say let us concentrate our efforts on further improvement of the dialysis. To my surprise, he agreed with me and immediately called his longtime friend Dr. Merrill and made an arrangement to send me to Boston to explore the possibilities. A few days later, I went to Boston for 10 days and Dr. Merrill taught me the basics of kidney transplantation. On the first day there, I was impressed to see a middle aged man who recently had a cadaver kidney transplant was walking in the hall with his wife. After coming back from Boston, Dr. Kolff and I organized our Kidney Transplant program. The first task was to name the transplant team. Many kidney transplant surgeons in the nation were all well-known general surgeons. Instead, Dr. Kolff chose our urologist Dr. Eugene Poutasse who had successfully done renal vascular surgery 14. He and another urologist Dr. Ralph Straffon did kidney transplants. Dr. Kolff and I would provide the clinical nephrological expertise, taking care of the patients before and after transplantation and the related donors. Dr. Donald Senhauser would do the pathology. The first committee meeting took place on November 27, 1962. We decided not to perform live donor kidney transplants until we got enough experience with cadaver kidney transplants.
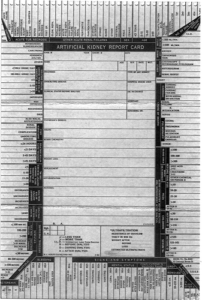
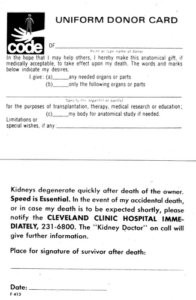
From 1959 to 1962, total body radiation therapy was used by Hamburger in Paris 15. In 1960, 6-mercaptopurine (6-MP) was first used by Calne 16. At CCF in the 1960s, the antirejection drugs were prednisone, azathioprine (Imuran), and actinomycin C. Only the first patient received local radiation (600r) to the allograft 17. To make a better selection of recipients and donors in 1962, tissue matching was developed by Paul Terasaki 18. In 1978, cyclosporine was used for the first time by Calne et al. 19. At CCF, the first kidney transplant was done using a cadaver donor on January 9, 1963 on a 48 year-old female who passed away on January 24, 1963. The second cadaver kidney transplant was done on January 18, 1963 on a 29-year-old man who died on January 23, 1963. Then on April 1, 1963, the first related living donor kidney transplant was done from a 40-year-old mother to a 14-year-old daughter and the recipient lived for many years without rejection. From January 1963 to the end of 1966, a total of 37 related and 101 cadaver donor kidney transplants were performed 20. In 1965, I received unexpected calls from Dr. John Merrill in Boston and Dr. David Hume in Richmond, VA. Both had trained at Brigham and Women’s Hospital. They mentioned the survival rate of cadaver kidney transplants were so poor that they were going to discontinue the transplants. The cause of death was overwhelming infection secondary to severe leukopenia. I told them our cadaver kidney transplant program is satisfactory, so that we are encouraged to continue the program. I then analyzed these contrasting results and realized after transplant their groups dialyzed recipients only when the BUN increased over 100 mg/dL. They believed a mild uremia acts as immune suppressive. Contrarily, we continued to dialyze the recipients twice weekly up to 4 weeks postoperatively, if the allografts did not function well. Then, the allograft biopsy was done to evaluate its pathology. If viable we continued dialysis. Otherwise, the allograft was removed. I then suspected Imuran is not bound 100% to serum protein. Thus, a significant amount of it was dialyzed out and severe leukopenia was avoided. Later my associate Dr. William Braun, tissue typing specialist, found that azathioprine is bound 30% to protein and is partially dialyzable. The second kidney transplant committee meeting was held on August 10, 1963 and the main discussed subjects were as follows: (i) Because of our interest on the relation of hypertension and bilateral nephrectomy, all patients had it on acceptance to the program, (ii) selection of related live and cadaver donor, and (iii) post operatively the recipient will be kept in the ICU for 7 days and then transferred to a private room. The caring staff needed maximal sterile technique to take care them. The third kidney transplant committee meeting was held on October 20, 1964. As we had successful kidney transplants from cadaver donors, it was decided to ask for procurement of cadaver donors from regional hospitals. The donor’s kidneys were to be removed in the operating room at each hospital. To transport cadaver kidneys in sterile condition, I made a small container from a paint spray can with the help of our own machine shop (Fig. 8). A 29-year-old man who had a cadaver kidney transplant on January 14, 1964 had lived for 18 years with normal renal function and then died of lymphoma. At that time, he was the longest cadaver kidney transplant survivor in the world. Figure 8 The fourth kidney transplant committee meeting was held on December 9, 1964 to discuss further details for obtaining cadaver donor kidneys from the regional hospitals and how to bring them to CCF. We asked the Coroner’s cooperation to remove kidneys from the victims of whose main cause of death was not related to kidneys and this was agreed to. Time was essential, so we asked for police escort. When we called the police station, it caused an unexpected logistic problem. Many news media were at the station awaiting any exciting news. It became the top evening news. At the beginning, CCF administration was not happy about this and thought we called the media for publicity. Local recognition of our work started with the publication of the CCF renal transplantation experience in the Cleveland Plain Dealer newspaper on May 1, 1964. On October 5, 1965, the issue of Life Magazine was dedicated to CCF’s kidney transplantation experience using cadaver donors. That article was entitled “The Gift of Life from the Dead” and had worldwide circulation and acceptance. Because of our success with cadaver kidney transplantation, the procurement of cadaver donors from other regional hospitals became a priority. In order to expand the procurement effort to other hospitals, Dr. Straffon and I attended their monthly staff meetings to educate them and request their help in this effort. In 1965, Dr. Kolff designed a Uniform Donor Card (Fig. 9) hoping that many people would carry the card in their wallets. Uniform Kidney Donor Card invented by Dr. Kolff in 1965. In 1963, the National Institutes of Health established a Task Force to create a national registry for kidney transplants 20. The members of the Task Force included Dr. Thomas Starzl from Denver, Dr. Joseph Murray from Boston, Dr. David Hume from Richmond, Dr. Keith Reemtsma from Salt Lake City, Dr. John Najarian from Minneapolis, Dr. Donald Martin from Los Angeles and myself from Cleveland. The NIH first asked Dr. Kolff to be a member but he recommended me because I had organized the program. The initial meetings of the Task Force were very lively and manifested the rivalries that existed between leaders of the different programs. The task force published three Kidney Transplant Registries from 1963 to 1969. The September 3, 1965 issue of Medical World News published the famous specialist team that provided the sophisticated patient care at CCF. Most doctors are research-minded, and staff members were encouraged to do both. The Medical World News showed pictures of Drs. Irvine Page, world known hypertension expert, Willem Kolff, inventor of the AK, George Crile Jr, a general surgeon, Mason Sones, pediatric cardiologist and inventor of coronary artery angiography, Ralph Straffon, a urologist who became the president of American College of Surgeons, and Rupert Turnbull, an expert on colon and rectal surgery. When I became a research associate in 1959, Dr. Kolff took me to the nearby Art Museum once a month for lunch to discuss a new research project as there were too may disturbances at his office. The museum had a small cafeteria where a simple lunch was served. We usually had a bowl of soup and sandwich at a quiet outside table. One example was that in the middle of 1961, we discussed the organization of our own kidney transplant program. Before leaving we looked at a couple of exhibitions. In 1969, the National Cadaver Donor Kidney Transplant Registry was founded in order to take advantage of tissue typing in the selection of donor–recipient pairs. In order to allow transporting donor kidneys to the best matched potential recipient, a reliable preservation system was needed. The first successful effort came from Dr. Fred Belzer in 1967 21 followed by others including Dr. Magnus Magnusson of the CCF 22. In those days, the most used preservation method in this country was simple flushing of the donor kidney followed by air transportation in a sterile closed transport container labeled clearly to be identified as a donor kidney. Finally, in order to honor my mentor for his vision and talent, I will conclude this writing by listing the many tasks that Dr. Kolff delegated to the fellows when receiving requests for his help from around the world: As chronic dialysis had become successful, in 1964 the NIH chose five hospitals in the nation and offered $125 000 grants each for Phase II chronic dialysis program. They were the University of Washington under Dr. Scribner, Brigham and Women’s Hospital under Dr. Merrill, Georgetown University in Washington, DC under Dr. George Schriner, the University of Colorado Medical School in Denver under Dr. Joseph Holmes and Dr. Kolff at CCF. However, the CCF administration refused it. As Dr. Kolff did not want this grant to go to other cities in Ohio nor other states, he invited his former fellow Dr. Victor Vertes who was at that time Chief of Medicine at Mount Sinai Hospital in Cleveland. The NIH accepted Dr. Kolff’s suggestion and the grant was given to Dr. Vertes. In 1965, Dr. Kolff was allowed by CCF administration to solicit a grant of $125 000 from the Hartford Foundation to support chronic dialysis at the CCF. It was granted and he established a six bed chronic dialysis unit. Dr. Kolff taught me general nephrology and clinical application of the AK. I admired and respected him as my teacher. His nickname was “Pim” and his children called him “Daddy-o.” He gave me life lessons too. One such lesson was always to have time for the family no matter how busy at work. He said “Never Neglect the Family.” He always emphasized the importance of children’s education. When he started at CCF in 1950, he was not making enough salary for his children’s education and had to borrow money from the bank. The four sons (Jack, Albert, Keas, and Thrus) attended the private University School in Gates Mills, OH and private Allegheny College in Meadville, PA. Jack, Keas, and Thrus became physicians. Unfortunately, Albert lost his right eye when he was a teenager. This accident happened while cutting wood with a power saw in his basement. He became a lawyer. After college, daughter Adrie served in the Peace Corp in Africa. In June 1967, Dr. Kolff was invited by his longtime friend, Dr. Keith Reemtsma, the Chief of Surgery at the University of Utah Medical School in Salt Lake City to join his program. At the CCF, his laboratory space was only half of the 6th floor research building. Dr. Reemtsma offered a new eight floor Research Building to continue a variety of artificial organ research including his beloved artificial heart program. He accepted and left the CCF in June 1967. I wanted to follow him but he advised me to stay here to grow the Dialysis and Transplant Programs that he and I had started. We became friendly competitors but maintained our friendship. He had purchased a 100-acre farm with a two story house in 1959 in Trumbull County, east of Cleveland and his family frequently stayed there over weekends. After moving to Utah in 1967, he had visited the farm once or twice yearly. I provided him transportation from and to the airport. He often stayed at our house. His last visit to the farm was in November 1999 and it was also his last stay at my house (Fig. 10). Figure 10 Dr. Kolff’s legacy can be measured in his inventions as well as the fellows who trained under him. I will mention a few: (i) After a year fellowship in 1960, Dr. Visith Sitprija moved to the University of Colorado and obtained a PhD in 1963. He went back to Bangkok in 1964 and became an associate dean at Chulalongkorn University Medical School as well as Chief of Nephrology, (ii) after a year fellowship in 1961, Dr. Jerry Rosenbaum who went back to Philadelphia and invented his hemoperfusion apparatus in 1971, (iii) after 3 years residency in internal medicine at CCF and a year fellowship under Dr. Kolff, Dr. Dudley Seto went back to Honolulu in 1962 and was the first nephrologist there. He introduced dialysis and kidney transplantation, (iv) after a year of fellowship in 1965, Dr. Julio Figueroa was invited to Ochsner Clinic in New Orleans to start a dialysis and transplant programs. He was well respected in the nephrology community and started the Regional Chapter in Louisiana for the National Kidney Foundation, and (v) after a year fellowship in 1965, Dr. George Dunea became a professor of medicine at University of Illinois Medical School in Chicago and also the head of nephrology at Cook County Hospital. Dr. Kolff gave me three mementos. The first one was a reproduction of a Renoir’s painting of Young Lady Arranging Her Earring. He gave me this just before he left for Utah. The second one was an oil painting by his German patient Anna Fell Rothstein under Nazi occupied Holland. The painting depicted the Red Square in Moscow and had an insert with the face of Josef Stalin. Third one was a 6 by 5 by 7-inch bronze statue of “Man on the Rotating Drum Kidney” (Fig. 11), which was made for Dr. Kolff in 1986 by his friend, Mr. D. Smith. The man on the statue is supposed to be Dr. Kolff himself. Mr. Smith made only 10 copies, one of which was given to me. Those three gifts are displayed at our living room in honor and remembrance of Dr. Kolff.
Figure 11 Dr. Kolff had received a total of 105 national and international awards and 12 honorary doctorates. In 1964, Carmeron Prize of University of Edinburgh, Scotland, in 1972 the Harvey Prize from Technion, in 1974 Orden de mayo at Merito en et Grado de Gran Offical, the Heights Civilian Award from the Argentine Government, in 1986 Japan Prize, in 1990 chosen as one of the 100 most important Americans of the century in the special Fall issue of Life Magazine and in 2002 the Albert and Mary Lasker Foundation award. He published more than 600 scientific papers including 5 books, 29 chapters, and 6 forewords in books. Dr. Kolff retired from the University of Utah in 1997 and moved to Port Townsend in Washington State to be close to his son Keas and his family. Dr. Kolff continued to be invited for lectures not only in the States but also foreign countries. In June 1999, he moved to Dunwoody Village, retirement community at West Chester Pike, Newton Square, PA at the outskirts of Philadelphia where his oldest son and his family lived. I called him once or twice a month over the telephone and we had exchanged Christmas cards every year. I still have 15 personal letters and 5 Christmas cards from him. He passed away on February 11, 2009 at the age of 97. He was so popular at the Village, the people there got together 3 months after his passing and celebrated his happy life. I have been fortunate to have Dr. Kolff as my mentor and collaborator at CCF for 11 fruitful years. That was the birth of a new medical specialty and I am fortunate to have been at the forefront of it with my mentor Dr. Willem Kolff. I am very thankful for his kindness to hire me as a research fellow in 1956, promote me to a research associate in 1959 and a staff physician in 1961. I retired in May 1991 after 35 years of service to CCF. I must emphasize that throughout Dr. Kolff’s illustrious career, he was always humble about his accomplishments. He told me that he was lucky that heparin and cellophane membrane were available. Otherwise, he could not invent the RDK in 1944.
Satoru Nakamoto was born in Yamaguchi, Japan in 1927. After having received his medical degree at Yamaguchi Medical School in Yamaguchi, Japan, he held intern and residency positions in Hawaii, New York City, Denver, and Cleveland, OH, USA. He served as Full Staff at the Cleveland Clinic Foundation from 1961 until his retirement in 1991.HOME DIALYSIS PROGRAM
ANTIREJECTION THERAPY


Biography