

Abstract
As a native Houstonian, the notoriety surrounding Dr. Denton A Cooley’s implantation of the total artificial heart on Good Friday, April 4, 1969, was inescapable. At the time, Drs. Cooley and Michael E. DeBakey were the two most famous surgeons in Houston and much of the world. They had worked together professionally for 18 years, revolutionizing cardiothoracic surgery and mastering aortic surgery from beginning to end. However, this working relationship ended abruptly, and one of the most famous feuds in medicine began. Little did I know at the time that I would train with both men, work in both their respective institutions (which are located on the most competitive block of the Texas Medical Center), and play a role four decades later as their relationship rekindled. Here, I recount what I have come to learn about these events.
The annals of medicine are full of famous feuds between physicians. Among those, however, few are as replete with all of the most challenging issues that present themselves in the development of cutting-edge medical procedures as the 40-year feud between physicians Denton A. Cooley and Michael E. DeBakey associated with the April 4, 1969 implantation of a total artificial heart (TAH) by Dr. Cooley into Haskell Karp. That surgery, which Dr. Cooley characterized as essential to save the life of a dying patient and which Dr. DeBakey characterized as immoral, improper, and childish, led to Federal and institutional inquiries, a lawsuit, and an irreparable rupture of the previously close working relationship of Drs. Cooley and DeBakey. Several months after this event, Dr. Cooley turned in his resignation as Baylor faculty to focus on building the Texas Heart Institute, which had broken ground 2 years before. Drs. DeBakey and Cooley had worked together professionally for 18 years, revolutionizing cardiothoracic surgery and mastering aortic surgery from beginning to end.
As a native Houstonian, the notoriety surrounding the implantation of the TAH was inescapable. In 1969, months before the Apollo 11 mission, Houston’s most famous citizens were arguably Drs. DeBakey and Cooley. My father was a lawyer at a local title company, and I was expected to follow in his footsteps as a junior in high school. There was no way to predict that my life would be entwined with both of these titans or that I would spend my whole career as a cardiothoracic surgeon on the most competitive block of the Texas Medical Center.
I was a college sophomore on break in 1971 when I secured a summer job as part of Dr. Cooley’s cardiopulmonary bypass pump team, just as the Texas Heart Institute was establishing specialty training in perfusion under Charlie Reed. On my first day, I watched Dr. Cooley repair an aortic arch on the ether screen; I was hooked on cardiothoracic surgery as a career afterwards. The volume of cases was staggering; 25–30 repairs per day were typical, and Dr. Cooley managed it all effortlessly, outworking his younger residents and fellows. I was fortunate to spend two summers with Dr. Cooley, which changed my life forever. I then attended medical school at the University of Texas Medical Branch in Galveston, much like Dr. Cooley had done.
In 1977, I met Dr. DeBakey when I returned to Houston for a general and vascular surgery residency at Baylor College of Medicine (BCM), followed by a thoracic surgery residency. Everything you have ever heard about being on DeBakey’s service is true. God help the man who pressed the wrong elevator button as every second mattered when caring for more than 100 patients in-house at Methodist Hospital. I loved every minute of it. Immediately upon completing my thoracic training, I was hired as an Assistant Professor of Surgery at BCM to join the “godfather of aortic surgery,” E. Stanley Crawford. I had the good fortune to work with Dr. Crawford for 7 years before his health failed; ultimately, I took over his practice and rose through the ranks at Baylor, eventually becoming Chief of the Division of Cardiothoracic Surgery in 2000.
I had several individual conversations with Drs. DeBakey and Cooley about the 1969 controversy over the years, and both were adamant that the TAH device was their own creation. In Dr. DeBakey’s case, one of our many conversations took place in the middle of the night at the airport in Beirut, as we were both leaving to return from Lebanon back to the United States. As for Dr. Cooley, we also had multiple discussions regarding the controversy of 1969. In 2005, I was tasked with relocating BCM’s Division of Cardiothoracic Surgery from The Methodist Hospital to St. Luke’s Episcopal Hospital and the Texas Heart Institute at the direction of the BCM Board of Directors. As a result, despite being full-time faculty at BCM, this move down the block on Fannin allowed me the opportunity to work closely with Dr. Cooley in his later years. Is it possible that both of these great men were right? Below, I recount the facts as I came to understand them, pieced together over nearly 50 years, starting in June 1972 when I attended the trial of Karp versus Cooley & Liotta.
In the late 1950s, Argentinian doctor Domingo Liotta and his brother Salvador Liotta developed a prototype tubular artificial heart using machinery from an airplane factory.1 Dr. DeBakey learned of their efforts while Dr. D. Liotta was observing at the Cleveland Clinic. In 1961, just at the dawn of cardiac valve replacement, Dr. DeBakey offered Dr. Liotta a surgical fellowship to help advance work on developing an artificial heart. He would be joining the recently recruited Dr. C. William Hall and other Baylor researchers (which in time grew to include a young Dr. O. Howard “Bud” Frazier). Dr. Liotta envisioned continuing his efforts to construct a workable TAH, especially after Dr. DeBakey secured extremely generous funding from the National Heart Institute (HE-05435). Ever the statesman, Dr. DeBakey finessed further collaboration with nearby Rice University, led by Dr. J. D. Hellums, Ph.D., Professor of Chemical Engineering. Dr. Liotta’s initial efforts centered on a tubular left ventricular assist device (LVAD) that bypassed the left ventricle going from the left atrium to descending thoracic aorta.2 Dr. Crawford implanted the Liotta-Hall intracorporeal heart bypass pump in 1963, but the patient only survived a few days. The development of the TAH over the next several years was fraught with challenges. Prototypes ranged from devices to replace only the ventricles after removing part of the heart to semi-implanted globular “assist” devices to biventricular devices. From Dr. DeBakey’s perspective, the LVAD device could provide much-needed aid to those patients recovering from cardiac failure from heart surgery. In 1966, he had tremendous success with a well-publicized report of a patient fully recovering from complex repair using temporary support from an LVAD.3 Despite Dr. Liotta’s perception that DeBakey’s focus on further developing the LVAD competed with efforts to advance the TAH, there were continuous efforts on both fronts. From January 30 to March 20, 1969, a biventricular prototype TAH was implanted in seven calves. Unfortunately, the first four died on the table, while the last calf, despite surviving for 44 h, never regained neurological function and was being pumped, as a cadaver.
Dr. Cooley, on the other hand, was contemplating his own research on artificial hearts at the Texas Heart Institute. In some ways, these efforts were directly related to his success with heart transplantation, which he first performed in May 1968, 6 months after Dr. Christiaan Barnard’s repair. Business was brisk; there was a scarcity of donor hearts, with Dr. Cooley resorting to using a sheep’s heart in one patient.4 In December 1969, Drs. Liotta and Cooley met to discuss the possibility of developing a TAH at the Texas Heart Institute; Dr. Cooley had always framed this meeting as initiated by Dr. Liotta. In a strategic and highly controversial move, Dr. Cooley brought Dr. Liotta on board, despite Dr. Liotta drawing his salary from Dr. DeBakey’s grant. Work was to be done off-hours (and for some, off-location in home garages) and privately funded (albeit a minuscule amount compared to the NHI). Dr. Cooley’s express purpose was to design a device that would only be used for temporary and lifesaving purposes and as a medium while a patient with complete heart failure was awaiting a transplant.
Haskell Karp, a 47-year-old printing estimator from Skokie, Illinois had suffered from heart ailments for 10 years. By his early forties, Mr. Karp had survived multiple heart attacks that left him with a weak and irreparably damaged heart. After having a syncopal episode in 1968, he had a Demand pacemaker implanted transvenously into the right ventricle. In the fall of 1968, he began to have frequent episodes of dyspnea, orthopnea, paroxysmal nocturnal dyspnea, and was progressing to congestive heart failure. He had severe three-vessel coronary artery occlusive disease, moderate pulmonary hypertension, and a left ventricular, left lateral, dynamic aneurysm confirmed by left ventricular angiography. He was referred to Dr. Cooley in Houston for further treatment and consideration of resection of the left ventricular aneurysm, with the possibility of a cardiac transplant or other interventions. Mr. Karp was admitted to St. Luke’s Episcopal Hospital on March 3, 1969, for evaluation as his heart was failing and scarcely capable of pumping enough blood to sustain his life. Notably, he was initially opposed to the idea of having a heart transplant.
By all accounts, Mr. Karp was at an acute risk of dying from heart disease unless radical measures were taken. Dr. Cooley felt that if he did not immediately operate on Mr. Karp, he would surely die while waiting for a transplant.
The plan was to schedule surgery to take out a wedge of diseased tissue from the left ventricle from Mr. Karp’s heart to reduce the abnormal size of his heart and allow it to pump more efficiently. Dr. Cooley explained to the Karps if this operation was not successful, he had a device that he could use as a temporary “bridge” until a suitable donor was found. There are multiple and conflicting accounts of what the Karps actually understood. According to Dr. Cooley, the Karps were aware and consented to the use of a TAH device as a last resort if all other treatments were exhausted. According to the Karps, they were reluctant to use the TAH device, and they may have understood the device to be similar to the cardiopulmonary bypass machine typically used during open-heart surgery.
On April 4, 1969, Mr. Karp’s overall cardiovascular condition was deteriorating, and word was delivered to Dr. Cooley that the operation should begin immediately. Dr. Cooley then performed a wedge procedure to remove a third of the anterior lateral scar, aneurysm, and a portion of the septum from Mr. Karp’s left ventricle. Mr. Karp required numerous defibrillations following the reconstruction because he simply did not have enough left ventricular function to sustain life. Dr. Cooley, assisted by Dr. Liotta and Dr. Robert D. Bloodwell, removed the heart and implanted the mechanical heart substitute per the backup procedure agreement.5 The entire procedure was filmed, including the moment shortly after Mr. Karp regained consciousness.
During this period, Dr. Cooley and Mrs. Karp made public appeals through the news media for a heart donor for a transplant. At one point, after identifying a donor, Mr. Karp was given large doses of immunosuppressant drugs to prevent rejection after the transplant. Sadly, when the donor heart arrived, it was not viable. Mrs. Karp then appeared on national television and requested a donor to save her husband’s life. On Easter Sunday, April 6, 1969, a potential donor was identified and flown in from Lawrence, Massachusetts. Mr. Karp was ready for the transplant 64 h after receiving the total artificial heart. The TAH was removed, and the transplanted donor heart was sewn in, and after one defibrillation, it began beating normally. Again, the procedure was filmed and ultimately released as a feature entitled “Staged Cardiac Replacement” (Figure 1, Video S1). Unfortunately, Mr. Karp died on April 8, just 32 h after his transplant, from sepsis caused by acute pneumonia in his right lung.6

FIGURE 1 An image from the surgical film “Staged Cardiac Replacement” (AVF-IC043-225).
The first stage (left) involved heart replacement by using a total artificial heart. After a donor heart was identified, the artificial heart as removed and a donor heart was transplanted in its place in the second stage (right). The entire video may be viewed at https://youtu.be/gnU1xogRa18. Used with permission from the Texas Heart Institute Film Collection, McGovern Historical Center, Texas Medical Center Library [Color figure can be viewed at wileyonlinelibrary.com]
Dr. DeBakey was entirely unaware of Dr. Cooley’s work on the TAH or the surgical procedure on Mr. Karp until after the operation was performed. In a case of epic timing, Dr. DeBakey was in Washington, DC, at the time of Mr. Karp’s surgery and meeting with Dr. Theodore Cooper, the director of NHI, regarding progress on the development of the TAH. It would be an understatement to say
Dr. DeBakey was livid at the news; the NHI had invested millions into BCM to support his research. Concerns were raised about the likely use of NHI funding for the development of the artificial heart used in Mr. Karp’s operation, as well as the concern that human-related project guidelines were not followed. Mr. Leonard F. McCollum, Chairman of the Board of Trustees of BCM, appointed a special committee charged with “the responsibility to investigate compliance by the college with the guidelines established by the National Heart Institute for the development and use of the artificial heart” (Figure 2, Video S2).
More than a dozen faculty and staff provided testimony to the committee. They determined the device was fabricated in the Baylor laboratory facilities, in the machine shop overseen by Mr. Louis Feldman, and in the plastic shop headed by Ms. Suzanne Anderson. They both testified that they had assembled approximately 15–16 pumps allegedly identical to the one placed in Mr. Karp, but three of the pumps were missing. Additionally, Ms. Anderson added that Dr. Liotta was anxious and irritable the weeks prior to the event and that she suspected the devices might be being prepared for human use. A member of the Rice University team created the driving console as an off-hours side project, with the permission of Dr. Hellums, but was denied permission to operate the console during the repair. The committee also concluded that Drs. Cooley and Liotta did not seek any form of institutional approval prior to use.

FIGURE 2 A spokesperson from Baylor College of Medicine provides an update on the Board of Trustees’ investigation into the use of the total artificial heart. From the KHOU-TV Film Collections (KHOU Box 6904 Reel 21). This video may be viewed at https://youtu.be/m7MYTsMiVhM. Used with express permission of the Houston Metropolitan Research Center at the Houston Public Library [Color figure can be viewed at wileyonlinelibrary.com]
The investigation highlighted the need for additional regulation of human research studies at BCM, shifting from the free-wheeling innovation of the 1950s and 1960s to more structured research. Originating from BCM’s Committee for Human Research, the college instituted new regulations regarding protocols for clinical trials, particularly surgical ones, which required faculty to sign a formal agreement. Dr. Cooley stated that he could not sign such an agreement in good conscience, and consequently, he resigned from the Baylor faculty in June 1969 to focus all of his clinical, research, and educational efforts on the Texas Heart Institute.
As with most things, there is more than one side to a story, and simplicity is never the general rule. This is especially true for the development of the TAH device as well as the driving console. There were some differences between the device used in Mr. Karp and the one produced by the DeBakey-Baylor Laboratory. Dr. Cooley’s device included Wada-Cutter prosthetic valves that he specifically purchased using his own resources. There were also other modifications which included materials to adapt the device to human anatomic considerations. In his report to the Baylor Committee, Dr. C. William Hall noted that in addition to having different valves, Mr. Karp’s pump outflow tract was slightly different. It was sutured around the valve area rather than being incorporated directly into the fabrication, with the final design modified somewhat. Additionally, considering that Dr. Liotta was previously a designer of artificial hearts, he likely based at least some of his BCM prototypes on his prior work. In 1971, after a brief stint at THI and elsewhere in Houston, Dr. Liotta returned home to Buenos Aires to become surgeon-in-chief of the cardiovascular service at the Italian Hospital.
Initially, Mrs. Karp had praised Dr. Cooley in the media, stating that “Dr. Cooley had done everything in his power using his ability in whatever facilities at hand to save her husband’s life.” There was a documentary broadcast on national television, one in which Mrs. Karp participated personally, and another documentary aired in the fall of 1969. Mrs. Karp later expressed shock in seeing her husband’s heart removed and was unprepared for such emotion despite her participation in the documentary. Because of this and pressure from her sons, an action was commenced against Dr. Cooley in the US District Court for the Southern District of Texas in Houston under District Judge Singleton. The action was subsequently dismissed by USDC Judge Singleton, stating, among other things, that no medical expert opinion was given to even suggest that Dr. Cooley or Dr. Liotta were negligent in any way with regards to their diagnosis or surgical technique or that any such alleged negligence was the proximate cause of Mr. Karp’s death. The plaintiff subpoenaed Dr. DeBakey to testify based on his expert opinion. The well-publicized purported tension and “feud” between Dr. DeBakey and Dr. Cooley would be highly inflammatory and serve no purpose other than to introduce complicating issues into the case before a jury.
In his deposition, Dr. DeBakey stated that he would neither provide a medical opinion on the Karp case nor willingly answer any hypothetical question arising from the facts of the case. To keep the trial from becoming too public, the court had Dr. DeBakey questioned in private chambers with all counsel present and with a court reporter. Dr. DeBakey maintained that he had not been employed to give an expert medical opinion; that he would not accept any employment in this case; that he had never examined Mr. Karp; that he had never seen Mr. Karp; that he would refuse to express any medical opinion concerning the treatment of Mr. Karp; and that he would not express any medical opinion based on hypothetical questions even if asked to do so. Dr. DeBakey also refused to express in court his expert opinion concerning any connection between Dr. Liotta or the Cooley–Liotta mechanical heart used in Mr. Karp.
Consequently, the court concluded that Dr. DeBakey lacked any evidence worth presenting to the jury and would not allow the plaintiff’s attorney to call Dr. DeBakey as a witness, creating a highly biased and contentious circumstance that would provide no benefit. Dr. DeBakey returned the $20.00 that the plaintiffs had attached to his subpoena. Additionally, the plaintiffs were unable to present proof that Dr. Cooley had improperly obtained informed consent. The defendants’ attorneys requested a summary judgment, which was granted, and the case was dismissed without going before a jury. The plaintiffs appealed the case to US Court of Appeals for the Fifth Circuit—493 F.2d 408 (5th Cir. 174) but were unsuccessful. The Supreme Court refused to hear the case, putting a stop to the allegations.
The investigation carried out by Baylor faculty ultimately concluded that Dr. Cooley had exceeded his medical authority and used the DeBakey-Rice device without permission. The American College of Surgeons and the NHI carried out separate investigations. Both organizations concluded that any physician should feel obligated under proper circumstances to do whatever was reasonable to save a patient’s life, especially in an emergency. In Cooley’s own words shortly after implanting the TAH, he stressed the role of the TAH as a backup device and bridge to heart transplantation(Figure 3, Video S3). In Dr. Cooley’s choice to perform the surgery, we see all the most challenging issues in modern medicine: To what ends can and should a physician go to save the life of a dying patient? Do legal
and institutional limitations on physicians impede the development of innovative procedures? Who owns medical innovation?
Despite the passage of time, the events surrounding the use of the Liotta-Cooley artificial heart remain of interest (Figure 4, Video S4). In 1978, the total artificial heart that Dr. Cooley placed in Mr. Karp entered the permanent collection of the Smithsonian Institution’s National Museum of American History, joining the Liotta-Hall LVAD donated by BCM. As Dr. DeBakey passed away on July 11, 2008, at the age of 99, and Dr. Cooley passed away on November 18, 2016, at the age of 96, we can never know their facts regarding the Karp case with absolute certainty. We can, however, celebrate the fact that despite their 40-year feud, Drs. Cooley and DeBakey buried the hatchet after Dr. DeBakey

FIGURE 3 Defending the use of the total artificial heart as a bridge to transplantation, Dr. Denton A. Cooley faces the press in Houston in April 1969. From the KHOU-TV Film Collections (KHOU Box 6904 Reel 21). This video may be viewed at https://youtu.be/sDoOc4P_ruo. Used with express permission of the Houston Metropolitan Research Center at the Houston Public Library [Color figure can be viewed at wileyonlinelibrary.com]

FIGURE 4 Video depicting Drs. Denton A. Cooley and Michael E. DeBakey reflecting on the events surrounding the 1969 use of the total artificial heart. Dr. Cooley justifies its use as necessary to save the life of a patient; Dr. DeBakey admonishes Dr. Cooley’s surreptitious use of the device. This video may be viewed at https://youtu.be/pHLMF93UTlM. Used with express permission of Dr.
O.H. “Bud” Frazier [Color figure can be viewed at wileyonlinelibrary.com]
underwent a proximal aortic repair for an acute type I aortic dissection at the age of 97 (Figure 5). I believe the fact that these two historical medical figures and pioneers of cardiovascular surgery reconciled after so many years gives us all hope.3 In personal, private conversations, they both assured me that spending so many years as fierce competitors no doubt enriched their individual contributions to cardiovascular surgery.
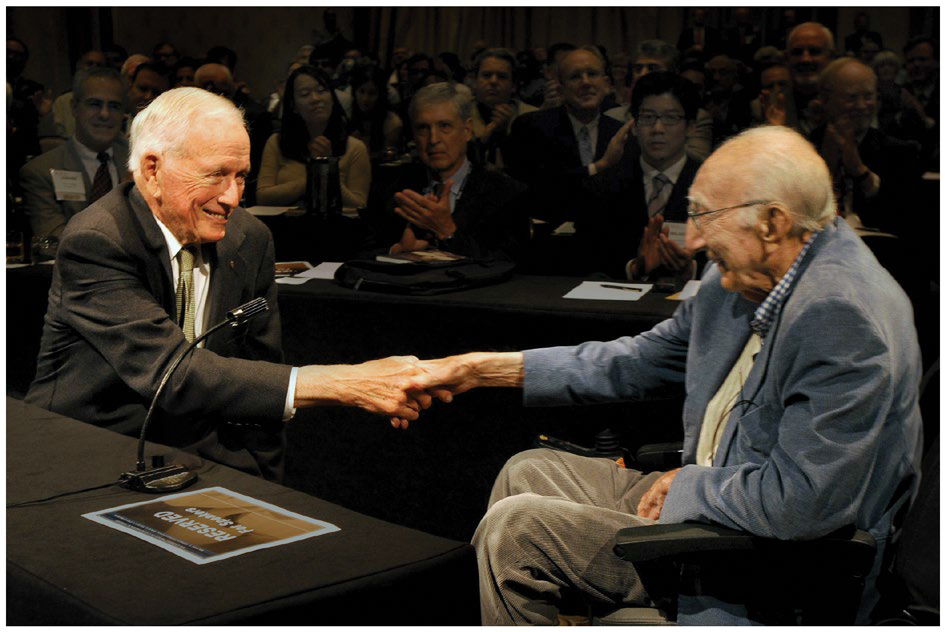
FIGURE 5 Photo of Dr. Michael E. DeBakey and Dr. Denton A. Cooley taken in 2008 in Houston, Texas. At the 2008 Joint Session of the 17th Congress of the Michael E. DeBakey International Surgical Society and the 6th Current Trends in Cardiothoracic Surgery Conference (meeting Director, Dr. Joseph S. Coselli), Dr. DeBakey honored Dr. Cooley with membership in the DeBakey Society. Photo taken by Agapito Sanchez. Used with permission of Baylor College of Medicine [Color figure can be viewed at wileyonlinelibrary.com]
ACKNOWLEDGMENT
Appreciation to Ginger Etheridge, BA, and Susan Y. Green, MPH, for editorial support. Special thanks to Dr. Bud Frazier for providing his recollections as well as video highlighting key aspects of this event.
CONFLICT OF INTERES T
Dr. Coselli participates in clinical trials with and/or consults for Terumo Aortic, Medtronic, and W. L. Gore & Associates and Edwards Lifesciences and receives royalties and grant support from Terumo Aortic. Dr. Coselli’s work is partly supported by an endowment from the Cullen Foundation.
Joseph S. Coselli1,2,3
1Division of Cardiothoracic Surgery, Michael E.
DeBakey Department of Surgery, Baylor College of Medicine, Houston, Texas, USA
2Department of Cardiovascular Surgery, Texas Heart Institute, Houston, Texas, USA
3Department of Cardiovascular Surgery, CHI St.
Luke’s Health—Baylor St. Luke’s Medical Center, Houston, Texas, USA
Correspondence
Joseph S. Coselli, Division of Cardiothoracic Surgery,
Michael E. DeBakey Department of Surgery, Baylor
College of Medicine, One Baylor Plaza, BCM 390,
Houston, TX 77030, USA.
Email: jcoselli@bcm.edu
REFERENCES
1. Liotta D, Taliani T, Giffoniello AH, Deheza FS, Liotta S, Lizarraga R, et al. Artificial heart in the chest: preliminary report. Trans Am Soc Artif Intern Organs. 1961;7:318–22.
2. Liotta D, Hall CW, Henly WS, Cooley DA, Crawford ES, DeBakey ME. Prolonged assisted circulation during and after cardiac or aortic surgery. Prolonged partial left ventricular bypass by means of intracorporeal circulation. Am J Cardiol. 1963;12:399–405.
3. Rosengart TK. The 1,000th VAD, the great rivalry, and the grand experiment of the Texas Medical Center. J Thorac Cardiovasc Surg. 2014;147:1745–7.
4. Cooley DA, Hallman GL, Bloodwell RD, Nora JJ, Leachman RD. Human heart transplantation: experience with twelve cases∗. Am J Card. 1968;22(6):804–10.
5. Cooley DA. First human implantation of cardiac prosthesis for staged total replacement of the heart. Trans Amer Soc Artif Int Organs. 1969;15:252–63.
6. Cooley DA. Recollections of the early years of heart transplantation and the total artificial heart. Artif Organs. 2011;35:353–7.
SUPPORTING INFORMATION
Additional supporting information may be found in the online version of the article at the publisher’s website.