

Originally published in Volume 37 Issue 10 of Artificial Organs, 20 October 2013

Ultrafiltration can be defined as filtration under pressure 1 through filters with minute pores 2, thus allowing the separation of large molecules from smaller ones 3. Ultrafiltration is often carried out using semi-permeable membranes. Such membranes are sometimes called differentially permeable membranes 4, permitting certain small-size molecules such as crystalloids but not larger ones such as colloids and suspending solids to pass through 1–3. Ultrafiltration has also been described as “the process of forcing out the solvent, with or without some of the solutes, through a semi-permeable membrane results in an increase in the concentration of the solutes that remain …” 5.
Types Of Ultrafiltration
Osmotic ultrafiltration
Two forms of ultrafiltration are often practiced in scientific settings. One, the osmotic ultrafiltration variety, depends on osmosis principles to bring about ultrafiltration. For example, Thalhimer used corn starch that possessed dextrose and dextrins as soluble osmotic agents on the external surface of a semi-permeable cellophane bag containing a serum sample. The aim was to abstract water and other small molecular weight substances from the contained serum so that the latter could be concentrated, thus fulfilling the criterion of in vitro osmotic ultrafiltration 6. Furthermore, in the course of hemodialysis in humans, Kolff and others enriched dialysates with large quantities of glucose to function as an osmotic agent in an effort to attract water and electrolytes from the blood into the dialysate, thus performing in vivo osmotic ultrafiltration 7, 8. Another example of osmotic ultrafiltration can be seen in peritoneal dialysis; such ultrafiltration is routinely carried out using glucose as a crystalloid osmotic agent and icodextrin as a colloidal osmotic agent 9.
Hydrostatic ultrafiltration
The other variety of ultrafiltration is known as hydrostatic ultrafiltration 10. This variety depends on the presence of a hydrostatic pressure or force gradient to induce the passage of a fluid across a semi-permeable membrane 10. The procedure can be performed in vitro or in vivo. When hydrostatic ultrafiltration is performed in vivo using an artificial kidney, one can use either: (i) the positive hydrostatic pressure method, with the positive pressure being applied on the blood side of the membrane 11 (e.g., by placing an adjustable clamp on the venous blood tubing of a dialysis circuit) 12, or (ii) the negative hydrostatic pressure method, with the negative pressure being exerted on the nonblood side of the membrane (e.g., by utilizing a sub-atmospheric pressure-generating mechanism through constricting the dialysate inlet tubing 7, 10, 12, bypassing of dialysate 13, use of a suction pump 14, and lowering of the dialysate drainage tubing to the floor below the dialysis patient to take advantage of the siphon effect 12). In the instance of the negative hydrostatic pressure technique, the total hydrostatic pressure exerted on the membrane, known as the transmembrane pressure, is the sum of the positive hydrostatic pressure exerted from the blood side and the negative hydrostatic pressure created from the nonblood side 15. The negative pressure procedure can be performed with or without the presence of a fluid on the nonblood side of the membrane. When performed during dialysis treatments, dialysate is present of course on the nonblood side (i.e., the dialysate side) of the membrane and the procedure is known as hydrostatic ultrafiltration during dialysis or ultrafiltration during dialysis. As ultrafiltration and dialysis are performed at the same time, this combined process has also been called combined dialysis and ultrafiltration 7 or simultaneous dialysis and ultrafiltration. When practiced in a clinical setting in the absence of a fluid (e.g., a dialysate) on the nonblood side of the membrane, the ultrafiltration procedure is commonly called IUF 14. It is of note that some of the means of producing negative pressure ultrafiltration mentioned previously apply to ultrafiltration during dialysis only, whereas some other means apply exclusively to IUF. The term “isolated” was coined because the procedure was carried out independently of (i.e., not at the same time as) any other process such as dialysis. From a therapeutic standpoint, IUF can be defined as “removal of fluid and molecular substances by convective transport through a semi-permeable membrane” 16. In this regard, certain general physical principles of hydrostatic ultrafiltration have previously been well described 17, 18.
It is noteworthy that prior to and for a short time after the publication of the definitions of ultrafiltration procedures in 1978 16, many authors often used the term hemofiltration to depict IUF 13.
In addition, in reviewing the older literature published before the term IUF was introduced, one needs to be cautious in deciding (if an author used the word “ultrafiltration”), whether he or she actually meant ultrafiltration during dialysis or IUF.
In 1856, Wilibald Schmidt in Bautzen, Germany 19 and Felix Hoppe in Strassburg 20 studied the filtration of different liquids enriched with gum arabic or proteins through membranes. While Schmidt used animal membranes for his experiments, Hoppe (later called Hoppe-Seyler) did his observations on peritoneal membranes in patients suffering from liver disease. They both became aware of the fact that solutions of colloidal bodies such as albumin, when filtered through membranes, produced filtrates that were less concentrated than the original solutions 19–22. Both found out that filtration depended on the applied mechanical pressure and the actual temperature. In 1896, C.J. Martin, by employing positive air pressures, successfully separated the proteins of serum and of egg white from salt solutions using gelatin or silicic acid membrane material as filters 22. Some years later, in 1907, Heinrich Bechhold employed filter paper impregnated with gelatin and hardened with formaldehyde or with collodion to perform filtration with the purpose of separating different colloids from one another 1, 23. By using various concentrations and combinations of gelatin, formaldehyde, or collodion, Bechhold could create membranes of different porosity 1, 23. By employing such membranes, it was possible to determine the mean size of various colloidal particles 22–24. By 1926, Arthur Grollman was able to further advance the knowledge of the physical chemistry and porosity of collodion membranes commonly used for ultrafiltration purposes 25.
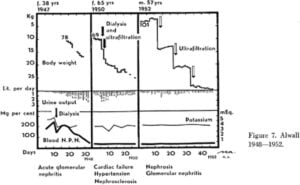
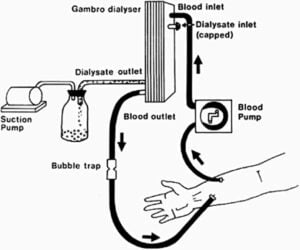
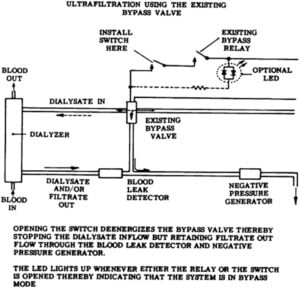
It was Lucien Brull of the University of Liege in Belgium, who first championed the performance of IUF in vivo on a dog in 1928 26. He devised an ultrafilter from a cooling apparatus made of an inner tube and an outer tube. The inner tube was punctuated with multiple holes and then covered with a piece of filter paper overlaid with collodion. This modified inner tube was then placed inside the outer tube. Heparinized blood from a dog’s carotid artery was routed through the inner tube. The hydrostatic pressure of the blood would bring about the passage of a plasma fluid through the covered holes of the inner tube into the lumen of the outer tube. The fluid so formed was an ultrafiltrate of the plasma 26. It is of note that no replacement fluid was given, so Brull did perform genuine IUF 14 rather than hemofiltration. In the latter procedure, replacement fluid is administered instead 27. In 1931, Alexander Geiger of the Hebrew University in Jerusalem used collodion membranes as components of a spiral, along with negative hydrostatic pressures to obtain ultrafiltrates from animals, performing in vivo IUF successfully. The aim of Geiger’s experiment was to compare the composition of an ultrafiltrate with that of the corresponding plasma 28. In 1947, Malinow and Korzon of the Michael Reese Hospital in Chicago were the first to use an ultrafilter consisting of cellophane tubes to perform hydrostatic ultrafiltration along with the administration of a replacement fluid in the form of a Krebs–Ringer solution for the purpose of removing uremic toxins from a dog 29. The dog’s own blood pressure was utilized as the driving force for blood to flow through the extracorporeal circuit. Seven liters of an ultrafiltrate was removed over 8 h, with the successful reduction of the serum urea nitrogen level from 175 to 75 mg/dL (62.5 to 26.8 mmol/L) However, because a replacement fluid was administered, Malinow and Korzon actually did carry out hemofiltration 27 rather than IUF, although the underlying basic principle of the ultrafiltration process was common to both procedures. In the late 1940s, Nils Alwall of Lund, Sweden, developed an artificial kidney in which a cellophane tubing was sandwiched between two closely adjacent mesh metal cylinders, allowing only a thin layer of blood to flow inside the tubing and restricting the expansion of the latter. As the entire cellophane tubing was placed in a tightly enclosed steel dialysate canister, a negative hydrostatic pressure in the form of a vacuum could be created inside the canister. As a result, ultrafiltration of the blood could be performed and regulated readily 12, 30, 31. In 1952, Lunderquist, a member of Alwall’s group, reported the successful removal of excess fluid from three overloaded patients by performing IUF using the above device and a suction mechanism. This approach was able to get rid of 1.4 kg of ultrafiltrate over 2 h in each of two patients, and 7.4 kg over 9 h in the third patient. The life-threatening pulmonary edema of this last patient was promptly mitigated 32. Indeed, in the early 1950s, Alwall and his colleagues did perform both IUF and ultrafiltration during dialysis on their fluid-loaded patients while fully realizing that those two procedures were distinct processes (Fig. 1) 12. Figure 1 From the late 1940s to the 1960s, dialyzers that featured plates, tubes, or capillaries, in addition to possessing enclosed dialysate compartments, began to be readily available. Examples of such dialyzers included the Skeggs-Leonards dialyzer, the MacNeill type dialyzer (e.g., the MacNeill-Collins dialyzer), and the Kiil dialyzer 33–43. Both the Skeggs-Leonards and the Kiil dialyzers were plate devices 33, 35 while the MacNeill-type devices possessed parallel straight cellophane tubes 34, 37. In all these dialyzers, the presence of a rigid, enclosed dialysate compartment allowed the ready generation of a negative hydrostatic pressure in this space by the use of a vacuum-creating mechanism so that IUF could be easily carried out. This latter negative hydrostatic pressure method, unlike its positive pressure counterpart described previously, was generally preferred while the occurrence of hemolysis as a result of this negative pressure procedure has not been of concern 38. However, it is noteworthy that a disadvantage of some of these early dialyzers was related to the fact that they had to be assembled and sterilized by their users prior to use 38, 39. Below are some of the studies involving the use of Skeggs-Leonards, MacNeill-Collins, and Kiil dialyzers. Skeggs et al. in 1952 reported on the successful removal of fluid from normal and edematous dogs by means of IUF using cellophane membranes 40. At times, these investigators replaced the ultrafiltrates retrieved with a salt solution. Consequently, Skeggs et al. were practicing not only IUF but also hemofiltration 26. In 1961, S. Anthone presented his diagram illustrating how he performed IUF using a MacNeill dialyzer at an American Society for Artificial Internal Organs meeting 44. In 1961, McLean and Clason presented their successful in vitro (on stored human blood) and in vivo (on dogs) results of IUF using MacNeill-Collins dialyzers 37. The group headed by Doyle in 1962 41 described their experience using the MacNeill dialyzer to perform IUF in humans. In addition to managing fluid-overloaded renal failure patients, Doyle’s group successfully treated the edema of congestive heart failure patients with IUF. The therapy was met with satisfaction in those cardiac patients who had become unresponsive to conventional medical therapy and in those cardiac patients who might be able to undergo corrective cardiac surgery if their cardiovascular decompensation could be brought under control on a temporary basis. Anthone and Anthone in 1963 applied a vacuum to the cellophane tubes of MacNeill-Collins dialyzers to carry out intermittent IUF procedures on nine chronically edematous patients suffering from renal or heart failure 42. For renal failure patients, by using the same dialyzer, a period of IUF could be followed by a period of dialysis so that too rapid ultrafiltration that might have occurred during the IUF phase could be tempered. The vacuum effect was able to remove, for example, 7.7 L in 7¼ h in one of the patients. Heart failure in the patients often showed improvements after IUF treatments. Moreover, diuresis, in some of the IUF-treated cardiac failure patients, would return with the resumption of diuretic therapy 42. In 1972, Kobayashi et al. in Japan reported the successful use of IUF to control fluid excess in maintenance hemodialysis patients 43. These investigators employed the Kiil dialyzer and created negative hydrostatic pressures with suction pumps. Starting in the early 1970s, pre-sterilized, ready-to-be used, plate or hollow-fiber dialyzers/ultrafilters with enclosed dialysate compartments became more popular. In the early 1970s, satisfactory results of IUF in patients using such devices were described by the groups headed by Khanna and Silverstein, respectively 45, 46. For fluid removal, Silverstein’s group used a special polysulfone hollow-fiber ultrafilter (with a single ultrafiltrate port) either in series with a dialyzer (the latter for the purpose of dialysis) or in a stand-alone IUF setting (i.e., without concomitant dialysis). Successful removal of excessive fluid was achieved in five overhydrated maintenance hemodialysis patients 46. In 1975, Ing et al. reported on employing IUF successfully either before a hemodialysis treatment (using the same plate dialyzer that was geared for the subsequent dialysis run) or on nondialysis days in eight dialysis patients suffering from volume overload 47. After the sealing of one of the two dialysate ports in a plate dialyzer that possessed an enclosed dialysate compartment, a negative hydrostatic pressure was applied to the dialysate compartment via the remaining dialysate port with the use of a vacuum pump (Fig. 2) 47. It was suggested that a similar ultrafiltration approach might also be appropriate for diuretic-resistant congestive heart failure patients 47. Several other publications also followed the initial report, including one showing that IUF could help to combat dialysis-related ascites 48–52. Figure 2 It was Bergstrom et al., however, who deserved all the accolades when, in 1976, he showed that rapid ultrafiltration was better tolerated when carried out alone (i.e., IUF.) rather than with simultaneous hemodialysis 53. Their original observation was fortuitously made when a hypotension-prone dialysis patient tolerated rapid ultrafiltration well when the dialysate was mistakenly allowed to bypass the dialyzer. Subsequent studies suggested that a fall in plasma osmolality with resultant entry of extracellular fluid into cells might be a likely cause for the poorer tolerance to fluid removal in the instance of ultrafiltration during dialysis 53. In this regard, an IUF-induced lower body temperature leading to a greater degree of vasoconstriction and a higher resultant blood pressure response has been thought to be the cause for the superior ultrafiltration tolerance of IUF over that of ultrafiltration during hemodialysis 54. Shinaberger et al. in 1978 described a modern technique of performing IUF by routing dialysate away from the dialyzer (i.e., bypassing the dialyzer) to generate a negative hydrostatic pressure (Fig. 3), in sharp contrast to the old-fashioned approach of using a vacuum pump 13. Lastly, since the late 1970s, myriad, innovative advances in IUF (such as slow continuous ultrafiltration 55) have been made, a testimony to the beauty and the ingenuity of the procedure’s original concept championed by the trailblazing pioneers of the 19th century and the early 20th century chronicled here. Figure 3 Finally, Robert H. Goddard said it the best: “It is difficult to say what is impossible, for the dream of yesterday is the hope of today and the reality of tomorrow.” 56.
The tremendous help given by Prof. Orly F. Kohn of the University of Chicago, Dr Joerg Vienken of Germany and the staff of the Loyola University Health Sciences Library in the preparation of this article is greatly appreciated. A graduate of the University of Hong Kong, Dr. Ing received his research training under the tutelage of Prof. Oliver M. Wrong at the Hammersmith Hospital in London. Dr. Ing is the founding president of the International Society for Hemodialysis and a professor emeritus of the Stritch School of Medicine, Loyola University Chicago in Illinois, USA.History of hydrostatic ultrafiltration
In vitro studies
In vivo studies
Acknowledgments
Biography